Meniscus Injuries & Tears
Office Location
Discover Dr. Kiritsis' Precision Shoulder Replacement
Dr. Kiritsis' Specialties
Schedule an Appointment with Dr. Kiritsis
Meniscal Tears and Injuries in Richmond, VA
Disorders of the Knee | Meniscus | Meniscal Tears and Injuries
The meniscus is a commonly injured structure in the knee. The injury can occur in any age group.
In younger people, the meniscus is fairly tough and rubbery, and tears usually occur as a result of a forceful twisting injury.
The meniscus grows weaker with age, and meniscal tears can occur in aging adults as the result of fairly minor injuries, even from the up-and-down motion of squatting.
This guide will help you understand
- where the meniscus is located in the knee
- how an injured meniscus causes problems
- what can be done for an injured meniscus
Anatomy
What is a meniscus, and what does it do?
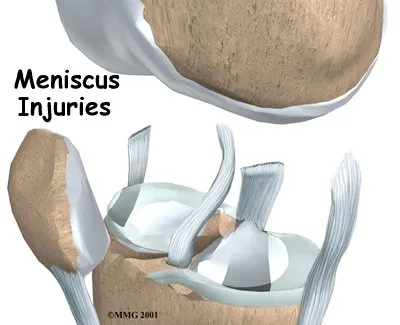
There are two menisci between the shinbone (tibia) and thighbone (femur) in the knee joint. (Menisci is plural for meniscus.)
The C-shaped medial meniscus is on the inside part of the knee, closest to your other knee. (Medial means closer to the middle of the body.) The U-shaped lateral meniscus is on the outer half of the knee joint. (Lateral means further out from the center of the body.)
These two menisci act like shock absorbers in the knee. Forming a gasket between the shinbone and the thighbone, help spread out the forces that are transmitted across the joint.
Walking puts up to two times your body weight on the joint. Running puts about eight times your body weight on the knee. As the knee bends, the back part of the menisci takes most of the pressure.
Articular cartilage is a smooth, slippery material that covers the ends of the bones that make up the knee joint. The articular cartilage allows the surfaces to slide against one another without damage to either surface.
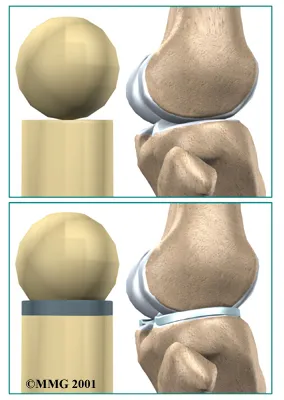
By spreading out the forces on the knee joint, the menisci protect the articular cartilage from getting too much pressure on one small area on the surface of the joint.
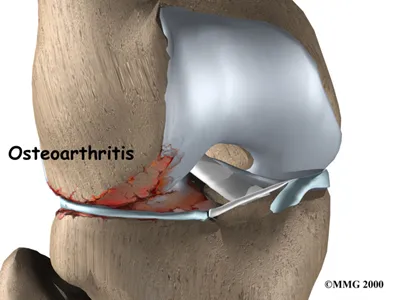
Without the menisci, the forces on the knee joint are concentrated onto a small area, leading to damage and degeneration of the articular cartilage, a condition called osteoarthritis.
The menisci add stability to the knee joint. They convert the surface of the shinbone into a shallow socket, which is more stable than its otherwise flat surface. Without the menisci, the round femur would slide on top of the flat surface of the tibia.
Related Document: A Patient’s Guide to Knee Anatomy
Meniscus Tears
A meniscus is a C-shaped cartilage found in the knee that helps conform the round surface of the femur to the relatively flat surface of the tibia. There are 2 menisci in the knee, the medial and lateral meniscus.
Their primary role is to absorb shock or disperse load that is applied to the knee during activities. Our knees see forces that exceed 4 to 7 times our body weight depending on the intensity of the activity.
Unfortunately, the meniscus has a poor blood supply which not only increases it’s susceptibility to injury but also diminishes it’s ability to heal. Once torn, the meniscus will have a decreased ability to absorb shock and will also become a source of pain in the knee. The posterior horn of each meniscus has the most pain fibers but the capsule of the knee also plays a role in the pain cycle of a meniscus tear. The lateral meniscus plays a larger role in absorbing shock than the medial side and injuries to this meniscus often make for a difficult recovery. In addition, complete loss of the lateral meniscus can increase the contact stresses up to 600% in the lateral side of the knee. A medial meniscus tear will also increase contact stresses. Unfortunately, whether you tear your medial or lateral meniscus your knee will be predisposed to developing arthritis in the future.
Treatment options consist of non-operative and operative treatment. Non-operative treatments include medicine (like Advil or Alleve), bracing, physical therapy, and maybe an injection. These treatments will not cure your tear but they may make it less symptomatic for you. I do worry about steroid injections into a knee that has a torn meniscus. I am concerned that the tear could not only become larger but may also cause damage to the articular cartilage “teflon coating” of the knee.
Surgical options include a meniscectomy and meniscal repair. Please see the meniscectomy video under the knee disorders section of my website. Meniscectomy is typically performed when the shape of the tear, quality of the tear or the vascularity of the tear are not conducive for a repair. I will typically perform a meniscal repair if I think the meniscus has a reasonable chance of healing. I will even be more aggressive with a repair in younger athletes. The recovery after a meniscectomy is typically much quicker and easier than with a repair. However, with any luck, a meniscus repair could restore your knees ability to absorb shock and reduce the risk of developing arthritis.
Causes
How do meniscal problems develop?
Meniscal injuries can occur at any age, but the causes are somewhat different for each age group. In younger people, the meniscus is a fairly tough and rubbery structure.
Tears in the meniscus in patients under 30 years old usually occur as a result of a fairly forceful twisting injury. In the younger age group, meniscal tears are more likely to be caused by a sports activity.
The entire inner rim of the medial meniscus can be torn in what is called a bucket handle tear. The meniscus can also have a flap torn from the inner rim.
The tissue that forms the menisci weakens with age, making the menisci prone to degeneration and tearing. People of older ages often end up with a tear as a result of a minor injury, such as from the up-and-down motion of squatting.
Most often, there isn’t one specific injury to the knee that leads to the degenerative type of meniscal tear. These tears of the menisci are commonly seen as a part of the overall condition of osteoarthritis of the knee in aging adults. Degenerative tears cause the menisci to fray and become torn in many directions.
Symptoms
What does a torn meniscus feel like?
The most common problem caused by a torn meniscus is pain. The pain may be felt along the edge of the knee joint closest to where the meniscus is located. Or the pain may be vaguer and involve the whole knee.
The knee may swell, causing it to feel stiff and tight. This is usually because fluid accumulates inside the knee joint. This is sometimes called water on the knee. This is not unique to meniscal tears, since it can also occur when the knee becomes inflamed.
The knee joint can also lock up if the tear is large enough. Locking refers to the inability to completely straighten out the knee. This can happen when a fragment of the meniscus tears free and gets caught in the hinge mechanism of the knee, like a pencil stuck in the hinge of a door.
A torn meniscus can cause long-term problems. The constant rubbing of the torn meniscus on the articular cartilage may cause the joint surface to become worn, leading to knee osteoarthritis.
Related Document: A Patient’s Guide to Osteoarthritis of the Knee
Diagnosis
How does Dr. Kiritsis identify this problem?
Diagnosis begins with a history and physical exam. Dr. Kiritsis will try to determine where the pain is located, whether you’ve had any locking, and if you have any clicks or pops with knee movement. X-rays will not show the torn meniscus. X-rays are mainly useful to determine if other injuries are present.
Magnetic resonance imaging (MRI) is very good at showing the meniscus. The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body.
This machine creates pictures that look like slices of the area. Usually, this test is done to look for injuries, such as tears in the menisci or ligaments of the knee. This test does not require any needles or special dye and is painless.
If there is uncertainty in the diagnosis following the history and physical examination, or if other injuries in addition to the meniscal tear are suspected, an MRI scan may be suggested.
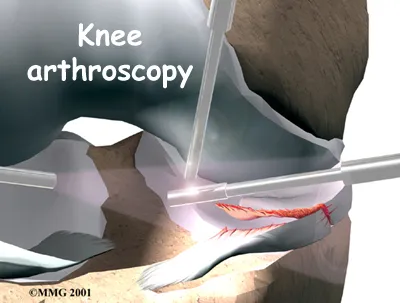
If the history and physical examination indicate a torn meniscus, arthroscopy may be suggested to confirm the diagnosis and treat the problem at the same time. Arthroscopy is an operation that involves inserting a miniature fiber-optic TV camera into the knee joint, allowing the Dr. Kiritsis to look at the structures inside the joint directly. The arthroscope lets Dr. Kiritsis see the condition of the articular cartilage, the ligaments, and the menisci.
Treatment
What can be done about this injury?
Nonsurgical Treatment
Initial treatment for a torn meniscus focuses on decreasing pain and swelling in the knee. Rest and anti-inflammatory medications, such as aspirin, can help decrease these symptoms. You may need to use crutches until you can walk without a limp.
Some patients may receive physical therapy treatments for meniscal problems. Therapists treat swelling and pain with the use of ice, electrical stimulation, and rest periods with your leg supported in elevation. Exercises are used to help you regain normal movement of joints and muscles.
Surgery
If the knee keeps locking up and can’t be straightened out, surgery may be recommended as soon as reasonably possible to remove the torn part that is getting caught in the knee joint.
But even a less severely torn meniscus may not heal on its own. If symptoms continue after nonsurgical treatment, surgery will probably be suggested to either remove or repair the torn portion of the meniscus.
Dr. Kiritsis uses an arthroscope (mentioned earlier) during surgery for an injured meniscus. Small incisions are made in the knee to allow the insertion of the camera into the joint.
Partial Meniscectomy
The procedure to take out the damaged portion of the meniscus is called a partial meniscectomy. Dr. Kiritsis makes another small incision. This opening is needed to insert surgical instruments into the knee joint. The instruments are used to remove the torn portion of the meniscus, while the arthroscope is used to see what is happening.
Dr. Kiritsis would rather not take out the entire meniscus. This is because the meniscus helps absorb shock and adds stability to the knee. Removal of the meniscus increases the risk of future knee arthritis. Only if the entire meniscus is damaged beyond repair is the entire meniscus removed.
Meniscal Repair
Whenever possible, Dr. Kiritsis prefers to repair a torn meniscus, rather than remove even a small piece. Young people who have recently torn their meniscus are generally good candidates for repair. Older patients with degenerative tears are not.
To repair the torn meniscus, the Dr. Kiritsis inserts the arthroscope and views the torn meniscus. Sutures are used to sew the torn edges of the meniscus together. Special fasteners, called suture anchors, may be used to bring the torn edges together.
Meniscal Transplantation
Surgeons are beginning to experiment with different ways to replace a damaged meniscus. One way is by transplanting tissue, called an allograft, from another person’s body. Further investigation is needed to see how well these patients do over a longer period of time. This procedure is reserved for patients under 40 years old that are symptomatic from a previous meniscectomy and have articular cartilage that is not significantly damaged.
Related Document: A Patient’s Guide to Meniscal Surgery
Rehabilitation
What should I expect from treatment?
Nonsurgical Rehabilitation
Nonsurgical rehabilitation for a meniscal injury typically lasts six to eight weeks. Therapists use methods such as electrical stimulation and ice to reduce pain and swelling. Exercises to improve knee range of motion and strength are added gradually. If your doctor prescribes a brace, your therapist will work with you to obtain and use the brace.
You can return to your sporting activities when your quadriceps and hamstring muscles are back to nearly their full strength and control, you are not having swelling that comes and goes, and you aren’t having problems with the knee giving way.
After Surgery
Rehabilitation proceeds cautiously after surgery on the meniscus, and treatments will vary depending on whether you had part of the meniscus taken out or repaired.
Patients are strongly advised to follow the recommendations about how much weight can be borne while standing or walking. After a partial meniscectomy, Dr. Kiritsis will instruct you to place a comfortable amount of weight on your operated leg using a walking aid if needed.
After a meniscal repair, however, patients will be instructed to keep their knee straight in a locked knee brace and to put only minimal or no weight on their foot when standing or walking for up to six weeks.
Patients usually need only a few therapy visits after a meniscectomy. Additional treatments may be scheduled if there are problems with swelling, pain, or weakness. Rehabilitation is slower after a meniscal repair or allograft procedure.
At first, expect to see the physical therapist two to three times a week. If your surgery and rehabilitation go as planned, you may only need to do a home program and see your therapist every few weeks over a six-to eight-week period.

Paul G. Kiritsis, MD
Dr. Kiritsis, a Richmond native, is one of a select number of Orthopedic Surgeons in the Richmond area to hold a second subspecialty board certification in Sports Medicine.